You can find answers to your questions about urinary system.
The kidneys are in the lumbar area close to the back and at the level of last two ribs. The kidneys are bean shaped and roughly fist sized. Their main function is regulate the water amount in the body, cleaning the blood by filtering and removing the metabolical waste by urine. In addition, they regulate blood pressure, control the production of blood cells and maintain bone growth.
The main working units in kidneys are filtering systems called nephrons. There are approximately 1 million nephrons in each kidney. The waste material coming to the nephron by arteries are filtered here. The produced urine pass through calyces and is collected at the center cavity of the kidney called pelvis and then removed from kidney.
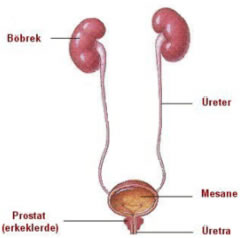
URETERS
The ureters are 25-30 cm long tubular forms placed between the kidneys and urinary bladder. They are mainly composed of muscle fibers. The urine formed in the kidneys reach the urinary bladder through these narrow tubes
URINARY BLADDER
The urinary bladder is a bag shaped expandable structure which is composed of heavy muscle fibers. When the urinary bladder gets full the muscle fibers forming the bladder walls are stretched and give the urge to urinate and when the bladder wall muscles are contracted the bladder is emptied.
URETHRA
This is the part of the urinary tract which connects the urinary bladder to the outside of the body. In females it is 3-4 cm long and in males it is approximately 20 cm long.
The stone disease has been known since 4800 BC, but, inspite of all the developments in technology the reason of stone disease is not perfectly known. The stone disease is accepted as a process where many interdependent factors are responsible. Some materials which are normally dissolved in the urine somehow precipitate and form crystals. In time, these crystals may combine and form the stones. Male cases are three times more common than females. The most common age group is 30-60 years old, however, stone formations can also be found in children.
Diet, hereditary factor, geographical location, frequent urinary tract infections, some metabolical anomalies and physical activity are among the factors effecting stone formation.
The climate can be a fascilitating factor for stone formation. In hot places and during summer, stone formation is more often. Increase in water loss due to perspiration resulting in decrease in urine amount and increase in urine concentration can make the precipitation of dissolved materials in the urine much easier.
Taking excessive amounts of purine, oxalat, calcium and phosphat with diet, drinking high mineral content water or extra hard water will cause removing of these materials from the body by urine and may cause stone formation.
Some hereditary metabolical anomalies (renal tubular acidosis, familial sistinuri) may be effective in stone disease.
It is accepted that regular exercise can decrease stone formation. Since family members share the same life styles, they may show similar stone disease.
Usually, the stone is composed of elements such as oxalat, calcium phosphate, uric acid, magnesium ammonium phosphate, sistin, xantin in pure form or in various compounds of these (mixed stone).
The most common of these elements in a stone are calcium oxalat and calcium phosphate.
Magnesium ammonium phosphate stones (Struvite stones – Infection stones) are more common in women and children. For formation of these stones, infection is necessary. They are usually in the shape of deer horn (koraliform – staghorn stone) and fill the cavities completely.
The uric acid stones are usually more common in people with high protein diet.
Sistin stones are formed due to metabolical defects and they are hereditary. Depending on the elements contained, the color of the stones can be white, yellow, brown, brick red or a combination of these colours.
Stones can be found anywhere in the kidneys and in the urinary tract.
The stones are generally in the sub-calix group (calix: the place in the kidney where the urine is first formed). The reason for this is that, in these places gravitational drainage of the urine is worse than other parts (for a normally standing person). The upper calix group is second in stone formation.
Stone formation starts in the wide parts of the calices and then stones which pass through the narrow calix neck reach the kidney pelvis with the urine. If the calix neck is very narrow the stone cannot pass to the kidney pelvis and continues to grow in that place. The properly sized stones which pass to the kidney pelvis reach the urinary bladder through the ureters. Big stones can be stuck in the kidney exits and anywhere in the ureter and cause blockage. In such cases there may be severe pain due to expansion and stretch of the kidney because of urine pressure. The stones which reach the urinary bladder can usually be easily expelled out. If there is any structural defect in the urinary tract or a urine blocking prostate (which is common in elder men), stones van cause blockage inside the urinary bladder or in the urethra (the part of the urinary tract which is after the urinary bladder). In these cases there may be symptoms of painful urination and blocking of urination.
The stones are usually round or ellipsoid. Their surfaces can be very smooth or rough or ragged with thorns. There may be different shaped stones in the same kidney. Sometimes the stones completely or partially fill the kidney cavity. Stones in the shape of deer horn are also called choraliform or staghorn stones.
Depending on their location the stones may cause different symptoms. The stones which are inside the kidney do not cause any major symptom as long as they do not block urine flow. They can cause symptoms like light pain in the lumbar area which increase with physical actvity, colour change in urine (red urine due to hemorrhage).
When the stones are somewhere between the kidney exit and urinary bladder, they block the urine flow heavily or lightly and can cause severe pain. Typically these pains sometimes get lighter, sometimes get more severe, but they never cease (colic pain). Mostly, symptoms like hemorrhage in the urine, nausea, vomiting, abdominal swelling and gas, pulsation in the kidneys accompany.
When the stones reach the lower parts of the ureter, they may cause pains in the pelvic area, urge to defecate, continous urge to urinate, burning and stinging feelings during urination.
Once the stone falls to the urinary bladder these symptoms are mostly reduced. There may be urge to urinate often, burning pain during the last part of urination, hemorrhage in the urine, blocking and hesitation to urinate.
When the stones which are somewhere in the kidneys and urinary tract cause infection, fever, chills, perspiration, fatigue, pulsating pain in the kidneys, severe burning feeling during urination, muddy and sometimes malodorous urine occur. These symptoms may show early stage of a simple urinary tract infection but also can show a very severe and serious condition called pielonephritis (kidney infection). Immediately consult to your doctor in sucah a case.
Since the stones is a fascilitaing factor for urinary tract infection, there will be relapses as long as the stones are not removed.
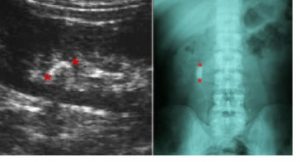
The first method to be used in searching for stones in kidneys and urinary tract is ultrasonography. A large majority of the kidney and urinary tract stones can be identified by this method. Ultrasonographic examination can sometimes be insufficient for small stones, urinary tract stones and in case of high amount of gas in the abdomen. Another method which is used often in searching stones is direct x-ray radiography or medicated radiography (IVP). In this method small stones and non calcium (non opaque) stones can not be identified. The golden method for searching stones is thin slice spiral tomography. All stones in the kidneys and urinary tract can be identified by this method. The disadvantage of this method is its imited use due to x-ray exposure of the patient.,
Stone treatment can be divided into 3 main groups:
1. Medical treatment
2. Extracorporeal stone breaking (ESWL)
3. Surgical method (Endoscopic method – Open surgery method)
The main approach in stone treatment is; wait for small stones to pass by themselves, follow-up by doctor as long as they do not cause any harm (even if there is no pain, there may be permanent, even irreversible damage in kidneys), if the stone grows or if it was so big when it was first detected and it will not pass by itself, use extracorporal stone breaking method to break the stone. When there is a stone which is not suitable for breaking, endoscopic or open surgery removal of the stone should be tried.
A doctor should decide which stone treatment method will be preferred depending on the patient’s condition.
1. Medical TreatmentPractically is it is not possible to dissolve or break a kidney or urinary tract stone (excepet a very small group) by medicine. Medicine treatment can be used for; to help the passing of stones which are at the right size for passing (especially those in the ureter), prevent growing of small stones or prevent reformation of stone after the stones are treated in any method (in patients who carry the risk of stone reformation)
In stone passing treatment, the first stage is to decide which stone can pass and which method should be used for which stone by your doctor. Then, the treatment is proceeded according to stone location, the condition of your urinary tract.
In order to have medicine treatment for preventing growth of existing stones, first the reason for stone formation should be known. Some urine and blood tests can be required for this.
Protection treatment will be discussed in following sections.
2. Extracorporeal Stone Breaking Treatment: (ESWL – Extracorporeal Shock Wave Lithotripsy)
This is the most modern stone treatment method which is painless and which does not have the risk for surgery. It has been first clinically applied in 1980 in Germany.
It is based on the principle of focusing an extracorporally sourced high frequency sound waves (shock waves) on a stone and breaking the stone. The equipment may be different according to the shock wave producing method (piezo-electric, spark gap, electromagnetic) or stone imaging method (ultrasonography, x-ray).
The shock waves focused on the stone cause surface erosion, and a stress wave which seperate structural elements of the stone and eventualy break the stone.
Previously, this method required a pool which the whole body is inserted in, ear protectors were used for protection from noise, and mostly anesthesia was necessary. Nowadays this method is very developed. The shock waves are transferred to body through a disk shaped tool or though a small pool where only the part of the body which the stone exist is inserted. There is no need for ear protectors. Anesthesia is very rarely necessary. Some advanced stone breaking equipments can also be safely used in baby-child patients. With the use of such equipments, the number of surgeries for stone treatment have been 90-95% decreased.
There may be differences in ESWL stone breaking equipments but they can be used for breaking stones anywhere in kidney, urinary tract and urinary bladder. For stones bigger than 3 cm, this method is not preferred as the first choice due to long treatment period, higher risk of complication. Complications (undesirable effects) of ESWL method are given below.
Hemorrhage area around the kidney (perirenal hematom):It is the most major complication. The occurrence percentage in small focused equipments is 0.6%, in big focused equipments 2-4%.
It is more common in patients with high blood pressure. Usually does not require any treatment, ESWL treatment should be suspended until the hemorrhage area is completeley healed. Rarely, the hemorrhage is not confined to kidney area and continues to enlarge. In these cases open surgery may be required.
Exposure to radiation:Not appliacble in equipments which has ultrasonographic imaging.
Bruise and tissue hardening (fibrosis) in kidney and in surrounding area due to shock wave. More common in big focused equipments, frequent and long treatment periods.
Stone pieces blocking the urinary tract (Ureter obstruction): The broken stone pieces may cause blockage in urinary tract. Sometimes a big stone at the front and sand following it may deposit. (Stone road) This case which is more common with big stones may be treated by breaking the big stone piece at the front.
3. Surgical Method
Surgical method can be simply divided into two groups; open surgery and removing the stone by endoscopic method.
The endoscopical method is becoming more important with advances especially in endoscopic equipments and increase in surgical experiences. Removing the stone by endoscopical method is done by either going in through the body’s natural openings (through the last prar of the urinary tract) or making a 1cm long cut in the skin and reaching the stone by going through the tissues (PCN- perkütan nefrolitotripsi). In order to remove the stone (big stone), once the stone is reached it may have to broken down. In this appliaction, depending on the size and location of the stone different stone breaking methods (mechanical, electrohydraulic, laser) can be used. There may be a possibility to continue with open surgery in each endoscopic operation.
In open surgery method, a surgical operation is done at an area depending on the location of the stone. It is the most accurate method in stone treatment. It has become less common due to risk of anesthesia, cut pain, risk of infection, constriction in the urinary tract, risk of urine leakage, long term confinement to bed. Nowadays, it is preferred in treatment of very big stones which are not suitable for other treatments, and cases which there are other structural anomalies in addition to stone.
Kidney or urinary tract stone may be a once in a lifetime case. However, more commonly it should be considered as a disease which requires constant effort to be protected from, which may cause permanent changes in the kidneys and in the urinary tract and which may be repetitive.
Since the reoccurence probabillity of stones in a patient with former stones in 3-5 years is 50%, we can see that protection is very important.
In protective treatment first the reason for stone formation should be known. Sometimes even with detailed laboratory tests the reason of stone formation can not be determined.
If there is a known metabolical anomaly, treatment for this is started.
In calcium stones, high intake of calcium with diet is not recommended. This does not mean totally removing calcium from diet. The main issue here is to prevent excessive calcium intake (usually more than 3 glasses of milk or equivalent). When determining the calcium intake amount, calcium removed with 24 hour urine should be kept within normal limits.
Since calcium is usually found as a compound with oxalat (calciumoxalat), restricting oxalat rich food and table salt is recommended for protection from calcium stones. Green leafed vegetables (spinach, beans, broad bean, green peas), beetroot, lemon, black grape, fig, strawberry, raspberry, blackberry, sour cherry, plum, walnut, nut, almond, tea, cacao, coffee, soda drinks and high dose vitamin C drugs increase the amount of oxalat in urine.
Calcium in urine increase because of osteoporosis. In patients with osteoporosis, tha calcium amount in urine can be controlled with osteoporosis prevention drugs.
In uric acid stones the uric acid amount in blood should be controlled. If the blood uric acid level is high, by a proper diet and medicine treatment the uric acid amount can be kept within normal limits and stone formation can be prevented. In a uric acid diet:
Never:
Alcohol, haslet, delicatessen goods, dried nuts, oat-oat flour, fish eggs, mussel, canned fish, broth. Sometimes Fish (prefer big fish), beef, lamb, sheep, chicken, turkey meat, mushroom: 60 hrdaily, Chickpea, dry beans, peas, lentil: 60gr daily, Spinach, cauliflower: 200 gr daily
In a group of patients with normal uric acid values, uric acid stone formation can be onserved. The PH of the urine is thought to be responsible for this. If the urine PH is higher than normal, which means more acidic, the uric acid amount dissolved in urine decreases and crystallisation starts. To prevent the stone formation in this group of patients, urine has to made neutral or more alkalic
In infection stones, treatment of infection is started. However, since the stone itself is a cause for infection, infection can’t be kept under control without removing the stone completely. Sistin crystals also dissolve in urine very lightly. To prevent sistin stone formation, urine has to be kept alkalic in sucah patients with proper medicine.
In addition to these, the patients should take plenty of fluid, have a medium level of physical activity and have periodical medical checks in order to prevent stone formation. According to the results of laboratory tests your doctor will help you by prescribing necessary nedicine.
Fluid intake (during summer 3-3.5 liters, during winter 2-2.5 liters) should be controlled so that daily urine amount shall be 1-1.5 liters. The more fluid intake the more urine amount and more diluted urine (more water content). So, the dissolved materials in the urine shall be less likely to form precipitation. By drinking more fluids, the small sand particles in the kidneys and in the urinary tract will be thrown out of the body without growing bigger.
In less active people little sand particles formed in the kidneys can more easily settle and grow bigger. Physical activity helps to throw out the sand particles mechanically.
By routine medical checks stone formation in kidneys and in the urinary tract can be detected at an early stage and proper treatments can be started. In this way, growing of the existing stones and making the treatment much harder and harming the kidney shall be prevented.


